Drugged Driving
Marijuana Impaired Driving
Driving under the influence of drugs (DUID) appears to be a growing factor in impaired-driving crashes. NHTSA’s 2013-2014 National Roadside Survey reveals a decreasing trend in alcohol use by drivers between 1973 and 2013-2014. By contrast, the percentage of weekend nighttime drivers who tested positive for the presence of marijuana rose from 8.6% in 2007 to 12.6% in 2014. While in 2013-2014, 8.3% of weekend nighttime drivers tested positive for alcohol (a BAC of more than .005) and 1.5% had a BAC of .08 or higher, 22.5% had a positive drug oral fluid and/or drug blood test; the survey focused on drugs with the potential to impair driving skills, including over-the-counter, prescription, and illegal drugs. The study does point out that the presence of drugs does not necessarily imply impairment. According to NHTSA, drug use among fatally injured drivers who were tested for drugs rose from 25% in 2007 to 42% in 2016, and marijuana presence doubled in this time frame.
Testing for drug impairment is problematic due to the limitations of drug-detecting technology and the lack of an agreed-upon limit to determine impairment. The nationally recognized level of impairment for drunken driving is .08 g/mL blood alcohol concentration. But there is no similar national standard for drugged driving. Drugs do not affect people consistently—a high concentration may significantly impair one person but not another. Drugs such as marijuana can also stay in the system for weeks, thus appearing in roadside tests while no longer causing impairment. In addition, tracking marijuana-impaired driving is difficult because drivers who may be under the influence of both marijuana and alcohol are often cited for a high blood alcohol concentration and rarely tested for additional substances.
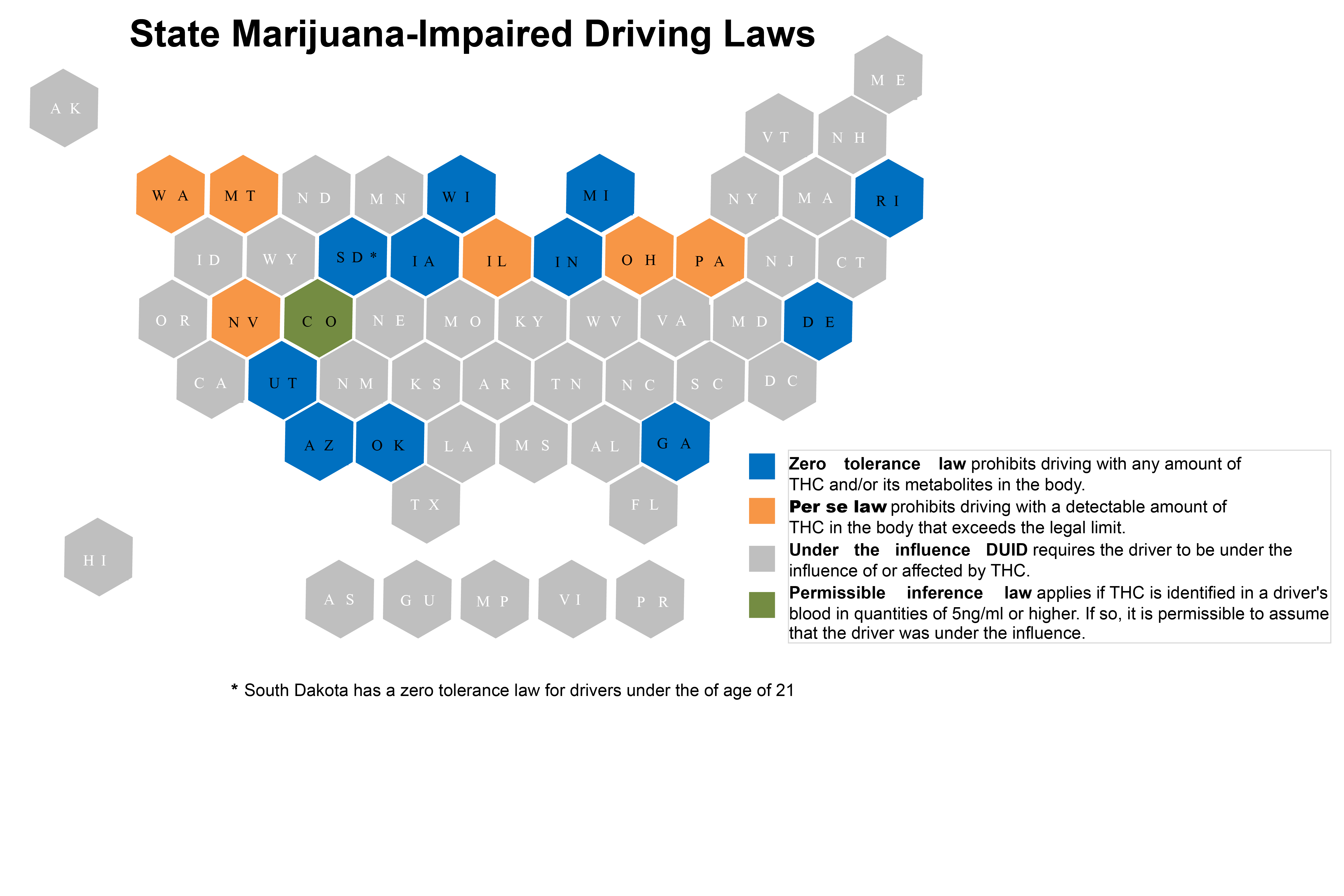
To address marijuana-impaired driving, every state has a law that, in some manner, deals with the issue (see below). Some states, including Alabama and Michigan, have permanent or active oral fluid roadside testing programs to screen drivers for marijuana and other drugs that could affect their behavior behind the wheel. Additionally, states are exploring methods to enhance driving under the influence of drugs (DUID) legislation and enforcement by better collecting crash and citation data.
- Fifteen states-Alaska, Arizona, California, Colorado, Illinois, Maine, Massachusetts, Michigan, Montana, Nevada, New Jersey, Oregon, South Dakota, Vermont and Washington-,Washington, D.C., Guam and Northern Mariana Islands permit recreational marijuana use. Thirty-six states, Washington, D.C., Guam, Puerto Rico and the U.S. Virgin Islands allow for comprehensive public medical marijuana/cannabis programs.
- Oregon legalized psilocybin (psychedelic plants) products for persons age 21 and older in 2020-becoming the first state to do so.
- Six states—Illinois, Montana, Nevada, Ohio, Pennsylvania and Washington—have specific per se limits for Tetrahydrocannabinol (THC), the component that gives cannabis its psychological effects and causes impairment, ranging between 1 nanogram and 5 nanograms. Per se laws establish that once a person is shown to have reached or surpassed the legal limit, that person will be considered impaired by law.
- Colorado’s reasonable inference law states that in instances where THC is identified in a driver’s blood in quantities of 5ng/ml or higher, it is permissible to assume the driver was under the influence. Reasonable inference laws differ from per se laws in that they allow drivers who are charged to introduce an affirmative defense to show that despite having tested at or above the legal limit, they were not impaired.
- Eleven states-Arizona, Delaware, Georgia, Indiana, Iowa, Michigan, Oklahoma, Rhode Island, South Dakota, Utah and Wisconsin-have zero-tolerance laws for certain drugs, including THC.
- New research from the AAA Foundation for Traffic Safety concluded that the number of drivers in Washington who test positive for marijuana after a fatal crash has doubled-from about 9% to about 18%-since the state legalized it in 2012. However, the authors pointed out that the study found only a correlation between legalization and an increased number of drivers involved in fatal crashes who tested positive, not a causative link.
- In Colorado, where recreational marijuana was also legalized in 2012, the number of fatalities in crashes in which drivers tested positive for THC rose from 18 in 2013 to 77 in 2016.
- AAA’s 2019 Traffic Safety Culture Index reveals most respondents consider driving shortly after using marijuana (70%) and driving after using potentially impairing prescription drugs (88.3%) to be very or extremely dangerous. Over 84% of surveyed participants support laws making it illegal to drive with a certain amount of marijuana in the driver’s system.
- Currently, the most common methods to detect marijuana are through blood, urine or saliva. However, some states have launched oral fluid testing pilot programs. Alabama, for example, initially conducted a pilot program and later transitioned to a permanent oral fluid toxicology program using oral fluid testing devices in both screening and evidentiary capacity. Michigan (Public Act 242 and 243 of 2016) gave authority to state police to develop an oral fluid pilot program. The initial pilot was conducted in five counties and used drug recognition experts to administer the oral fluid test. Unlike previous programs (like the three-year pilot program in Colorado that was started in March of 2015), this program was not voluntary as drivers were not given the option of opting out from providing a sample. Refusal to submit to an oral fluid test was considered a civil infraction. The program was extended for one year until Sept. 30, 2020, and is now conducted statewide.
credits: https://www.ncsl.org/research/transportation/drugged-driving-overview.aspx